Eyelid
Ptosis Treatment & Surgery
Surgical and non-surgical ptosis treatment — Müller's-muscle resection (Putterman), levator advancement, frontalis sling, Fasanella-Servat, and Upneeq eye drops.
Medically reviewed by Tamara R. Fountain, MDOculoplastic SurgeonLast updated June 2026
Part of our complete guide to Ptosis (Droopy Eyelid) — this page covers ptosis treatment and surgery in depth.
Treatment of Ptosis
The choice of operation depends on three factors: the degree of ptosis, the remaining levator function, and the phenylephrine test result. Dr. Fountain reviews all options with you at consultation and tailors the approach to your anatomy and goals.
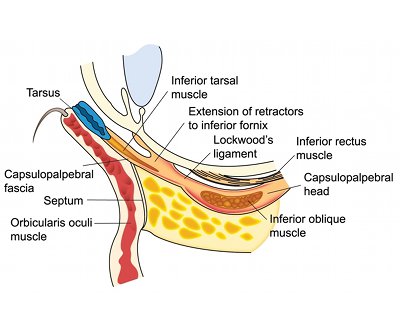
Müller Muscle–Conjunctival Resection (MMCR — Internal Approach)
- Incision made through the inner conjunctival surface of the lid — no external scar
- Best candidates: good levator function (≥ 10 mm) and a positive phenylephrine test
- The amount of Müller muscle and conjunctiva resected is determined by a formula based on the phenylephrine response
- Typically performed under local anesthesia with light sedation; because the resection amount is set by the phenylephrine-based formula, no awake intraoperative adjustment is required
- Can be combined with cosmetic upper blepharoplasty
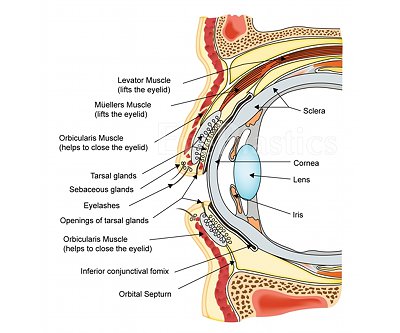
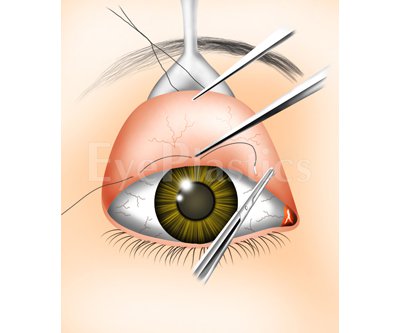
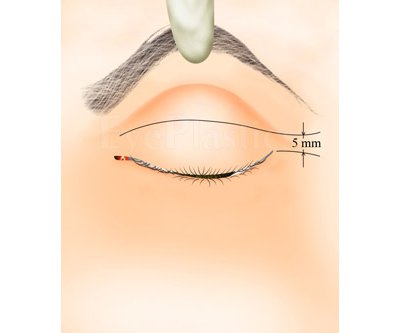
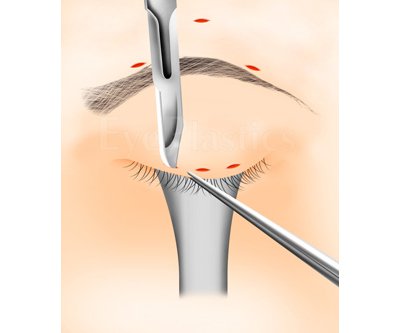
Levator Advancement (External Approach)
- Incision placed within the upper lid crease — scar is hidden in the natural skin fold
- The aponeurosis is reattached or tightened to the tarsus under direct vision
- Patient is awake during the key adjustment step so lid height and contour can be refined in real time
- Preferred for aponeurotic ptosis with moderate-to-good levator function
- Can be combined with cosmetic upper blepharoplasty through the same incision
Frontalis Sling
- The eyelid is suspended directly from the frontalis (forehead) muscle using a sling material
- Required for severe ptosis with poor levator function (≤ 4 mm) — the typical situation in congenital ptosis and Marcus Gunn jaw wink. Congenital ptosis carries roughly a 30% risk of amblyopia (from lid occlusion or induced astigmatism), so affected children need prompt pediatric ophthalmology evaluation
- Sling materials include autogenous fascia lata (harvested from the thigh), silicone rod, or Gore-Tex
- The patient opens their eye by raising their brow, not by contracting the levator
- Some lid lag on downgaze and lagophthalmos (incomplete lid closure on attempted closure and during sleep) are expected; lubricating eye drops/ointment are needed long-term
- Performed under general anesthesia; lid height is determined by a surgical formula
Ready to discuss Ptosis Treatment & Surgery?
Schedule a consultation with Tamara R. Fountain, MD to learn if this procedure is right for you.