Eyelid
Ptosis Evaluation & Diagnosis
How a droopy eyelid is evaluated — margin reflex distance, levator function, the phenylephrine (Neo-Synephrine) test, Hering's law, and visual-field impact.
Medically reviewed by Tamara R. Fountain, MDOculoplastic SurgeonLast updated June 2026
Part of our complete guide to Ptosis (Droopy Eyelid) — this page covers ptosis evaluation and diagnosis in depth.
Evaluation of Ptosis
Careful measurement is the foundation of ptosis surgery planning. Dr. Fountain records the following at every ptosis evaluation:
Video: What a Ptosis Evaluation Looks Like
- Margin-reflex distance (MRD-1): the distance from the corneal light reflex to the upper lid margin in primary gaze. Normal ≈ 4–5 mm; ptosis is present when MRD-1 is < 2 mm
- Levator function: total lid excursion from full downgaze to full upgaze with the brow held still. Excellent ≥ 10 mm; fair 5–9 mm; poor ≤ 4 mm — this single measurement largely determines the surgical approach
- Lid crease height: the distance from the lash margin to the skin crease, which guides the incision level
- Phenylephrine test: a drop of 2.5% phenylephrine behind the upper lid stimulates Müller’s muscle; elevation of ≥ 1 mm predicts a favorable response to internal ptosis repair (MMCR)
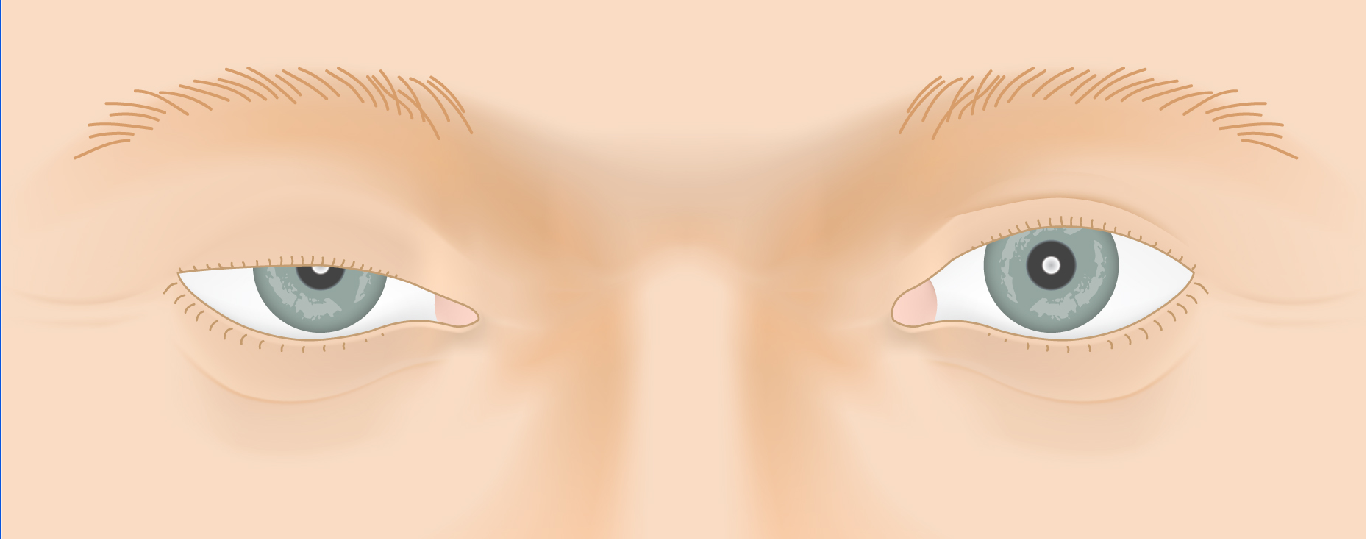
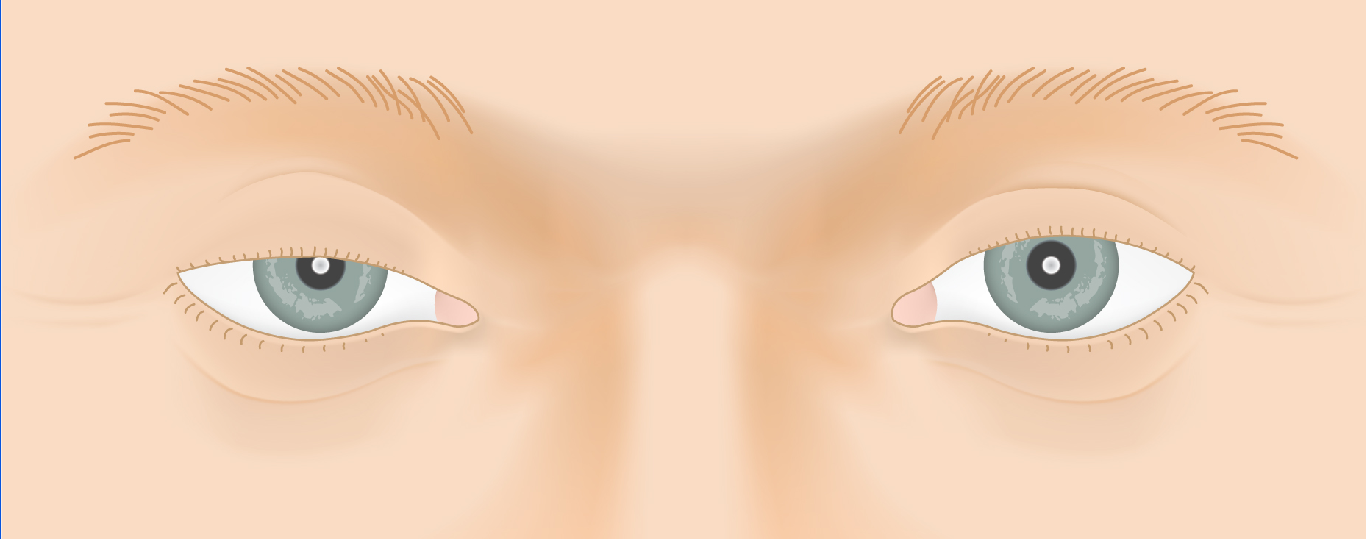
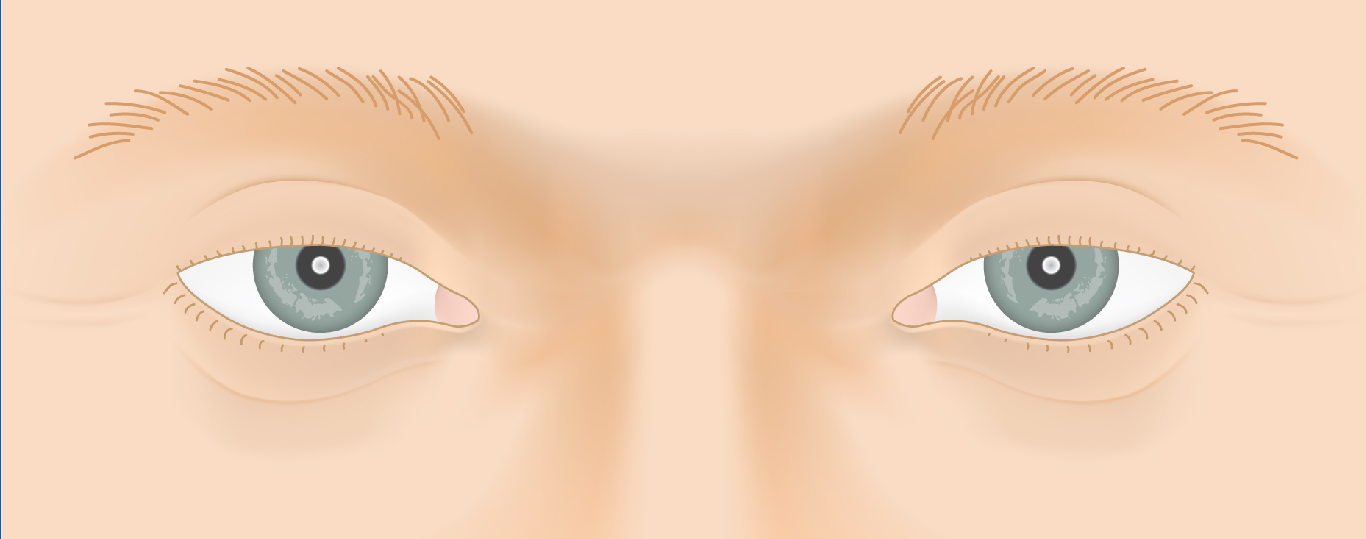
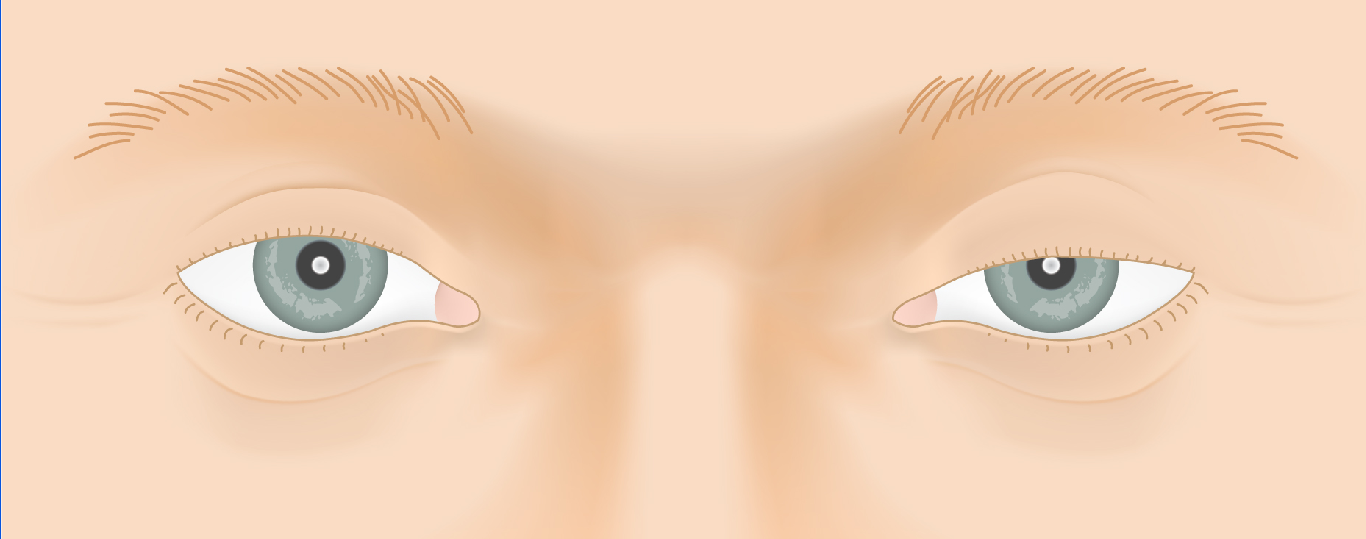
Hering’s Law of Equal Innervation
When ptosis affects only one eye — or is much worse on one side — Hering’s law becomes critical to surgical planning. Both levators receive equal central drive from the brain. In unilateral ptosis, the brain increases drive to both sides to keep the ptotic lid open. If surgery elevates the ptotic lid, that extra drive drops — and the fellow lid may fall.
This “see-saw” effect means apparent unilateral ptosis can unmask bilateral ptosis after surgery on one side. The interactive animation below demonstrates this phenomenon.
Ready to discuss Ptosis Evaluation & Diagnosis?
Schedule a consultation with Tamara R. Fountain, MD to learn if this procedure is right for you.