Orbital
Thyroid Eyelid Retraction & Double-Vision Surgery
Rehabilitative surgery for thyroid eye disease — correcting eyelid retraction and the restrictive strabismus that causes double vision, after the orbit is stable.
Medically reviewed by Tamara R. Fountain, MDOculoplastic SurgeonLast updated June 2026
Part of our complete guide to Thyroid Eye Disease (TED) — this page covers TED eyelid and strabismus surgery in depth.
Once thyroid eye disease has stabilized, two of its most disabling effects — a retracted, staring eyelid and double vision from tight eye muscles — are corrected surgically. These are the rehabilitative steps that follow orbital decompression.
Eyelid Retraction
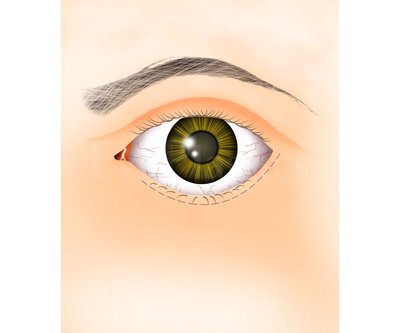
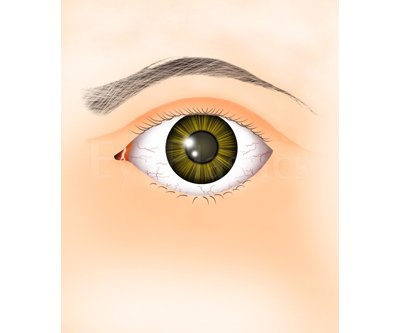
Eyelid retraction is among the most common and distressing features of TED. The upper lid normally covers 1–2 mm of the superior limbus; in TED it may sit above the limbus entirely, exposing the sclera and giving the characteristic staring appearance.



Causes of Upper Lid Retraction in TED
- Overactive sympathetic tone (Müller muscle stimulation from hyperthyroidism) — often partially reversible with thyroid control
- Levator muscle fibrosis — the levator becomes adherent to surrounding tissues; responds only to surgery
- Inferior rectus restriction with compensatory upgaze effort — increased levator drive to elevate the globe worsens lid retraction; strabismus surgery may reduce this component
Consequences
- Corneal exposure: dryness, punctate keratitis, corneal ulceration in severe cases
- Lagophthalmos (inability to close lids fully during sleep)
- Significant cosmetic distress
Surgical Correction
Eyelid surgery is the last step in the sequential rehabilitation of TED (after decompression and strabismus if needed), performed once disease is stable for ≥ 6 months.
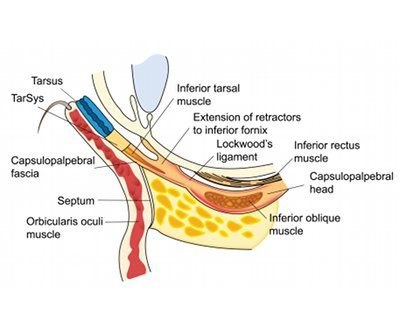
- Upper lid lowering: Müller muscle recession (müllerectomy), levator recession, or eyelid spacer graft (using donor sclera, hard palate mucosa, or synthetic spacer) to lengthen the posterior lamella. Can lower the upper lid by 2–8 mm depending on technique
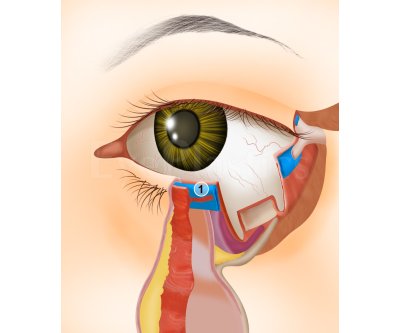
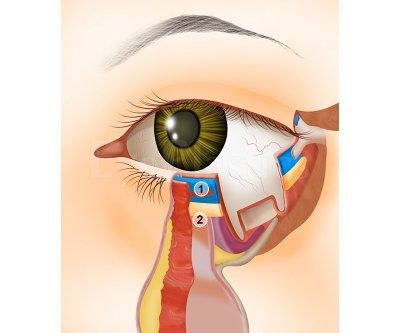
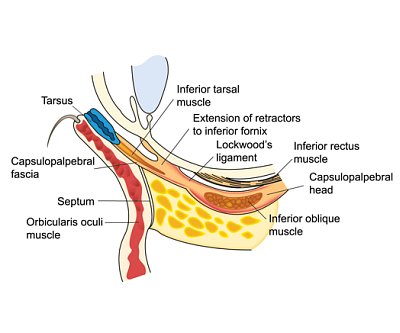
- Lower lid raising: Recession of the lower lid retractors with or without a spacer graft. Lateral tarsal strip canthoplasty to improve lower lid position and support
- Tarsorrhaphy: Partial closure of the lateral eyelids as a temporary or permanent measure for severe corneal exposure when definitive surgery is not yet possible
The animation below steps through the surgical correction of lower-eyelid retraction — recession of the lower-lid retractors, with or without a spacer graft — via both the external (transcutaneous) and internal (transconjunctival) approaches.
Ready to discuss Thyroid Eyelid Retraction & Double-Vision Surgery?
Schedule a consultation with Tamara R. Fountain, MD to learn if this procedure is right for you.